The World Health Organization’s International Classification of Functioning, Disability and Health (known as the ICF)1 is helpful for thinking about the role of rehabilitation in HIV.2-4
Health conditions (the top box) are often the focus of HIV care and treatment, whereas the ICF calls attention to the wide range of the life-related challenges resulting from health conditions that can be addressed by rehabilitation (boxes 3-5).
The model was designed for all types of diseases and functioning, not just HIV. It offers a common language for clinicians, managers, policy makers or others interested in models of care.
Figure 1.3: The ICF Model
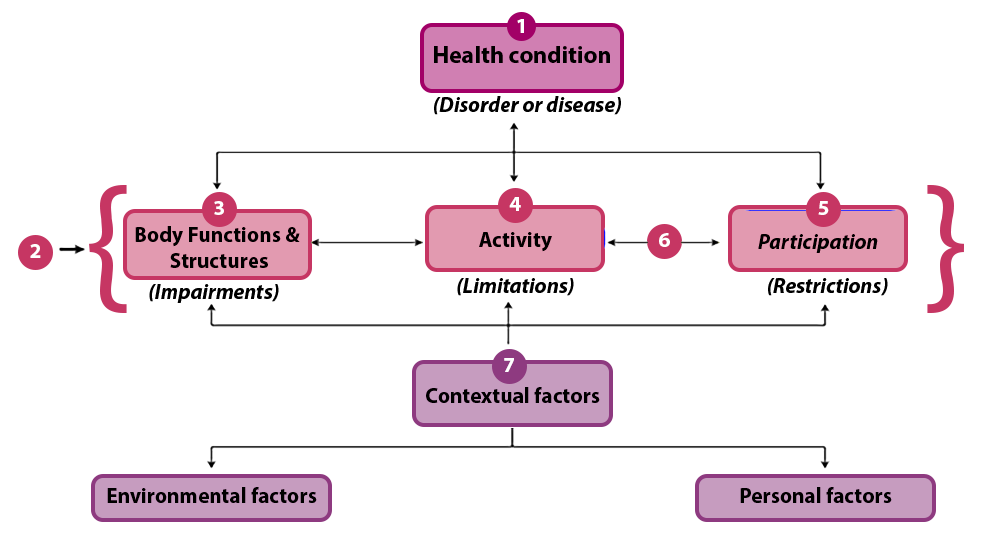
Figure 1.3: The ICF Model – Description
The model has four rows.
On the top row is a box titled Health Conditions (Disorders or Diseases).
This box describes the medical diagnoses, diseases or injuries that a person can experience. For a person living with HIV, this could be any combination of:
- HIV (e.g., the virus directly targeting the immune or neurological systems)
- HIV-related conditions (e.g., TB, pneumocystis carinii pneumonia, Kaposi’s sarcoma)
- Diagnoses related to ART (e.g., peripheral neuropathy)
- Diagnoses unrelated to HIV (e.g., multiple sclerosis, trauma resulting from a motor vehicle accident)
The second row contains three boxes. This row describes the life-related impacts that result from health conditions. Rehabilitation addresses these impacts.
The three boxes of life related impacts are:
Box 1: Impairments are problems in body function (physiological or psychological functions of body systems) or structure (anatomical body parts), e.g., weak abdominal muscles, memory loss, right-sided hypertonicity, congested lungs
Box 2: Activity limitations are problems executing a task or action (e.g., getting dressed, walking to a clinic, carrying one’s child, communicating with a neighbor)
Box 3: Participation restrictions are problems an individual may experience with involvement in life situations (e.g., being excluded from school, difficulty participating with one’s church, feeling stigmatized at work, challenges with parenting)
Issues at this level are bi-directional. This means that a challenge at one level can affect any other level. For example:
Peripheral neuropathy (health condition) causing bilateral leg pain (impairment) can limit one’s ability to walk to one’s bank (activity limitation) which in turn can limit one’s ability to manage their household finances (participation restriction).
Stigmatization for being HIV-positive can result in being excluded from one’s football team (participation restriction) which results in less physical activity (activity limitation) which results in decreased endurance and strength (impairments)
The third level represents contextual factors.
Contextual factors influence or shape people’s experiences with these life-related impacts of health conditions.
Environmental factors are the physical, social and attitudinal environment in which people live and conduct their lives (e.g., stigmatizing attitudes about HIV, stairs vs. ramp outside a health clinic, laws that criminalize certain HIV-related behaviours). These contextual factors include the social determinants of health (e.g., housing, food security, access to employment).
Personal factors are internal to each individual (e.g., gender, age, coping styles, education, past medical history).
Figure 1.3: The ICF Model Explained
| Box Number | Description |
|---|---|
| 1 | This box describes the medical diagnoses, diseases or injuries that a person can experience. For a person living with HIV, this could be any combination of:
HIV (e.g., the virus directly targeting the immune or neurological systems) HIV-related conditions (e.g., TB, pneumocystis carinii pneumonia, Kaposi’s sarcoma) Diagnoses related to ART (e.g., peripheral neuropathy) Diagnoses unrelated to HIV (e.g., multiple sclerosis, trauma resulting from a motor vehicle accident) |
| 2 | This row describes the life-related impacts that result from health conditions. Rehabilitation addresses these impacts. |
| 3 | Impairments are problems in body function (physiological or psychological functions of body systems) or structure (anatomical body parts), (e.g., weak abdominal muscles, memory loss, right-sided hypertonicity, congested lungs) |
| 4 | Activity limitations are problems executing a task or action (e.g., getting dressed, walking to a clinic, carrying one’s child, communicating with a neighbor) |
| 5 | Participation restrictions are problems an individual may experience with involvement in life situations (e.g., being excluded from school, difficulty participating with one’s church, feeling stigmatized at work, challenges with parenting) |
| 6 | Note the arrows are bi-directional. This means that a challenge at one level can affect any other level. For example:
Peripheral neuropathy (health condition) causing bilateral leg pain (impairment) can limit one’s ability to walk to one’s bank (activity limitation) which in turn can limit one’s ability to manage their household finances (participation restriction). Stigmatization for being HIV-positive can result in being excluded from one’s football team (participation restriction) which results in less physical activity (activity limitation) which results in decreased endurance and strength (impairments) |
| 7 | Contextual factors influence or shape people’s experiences with these life-related impacts of health conditions.
Environmental factors are the physical, social and attitudinal environment in which people live and conduct their lives (e.g., stigmatizing attitudes about HIV, stairs vs. ramp outside a health clinic, laws that criminalize certain HIV-related behaviours). These contextual factors include the social determinants of health (e.g., housing, food security, access to employment). Personal factors are internal to each individual (e.g., gender, age, coping styles, education, past medical history). |
1 World Health Organization: International Classification of Functioning, Disability and Health (ICF) – Geneva. 2001.
2 Myezwa H, Stewart A, Musenge E, Nesara P. Assessment of HIV-positive in-patients using the International Classification of Functioning, Disability and Health (ICF), at Chris Hani Baragwanath Hospital, Johannesburg. AJAR. 2009; 8(1):93-106.
3 Myezwa H, Buchalla C, Jelsma J, Stewart A. HIV/AIDS: use of the ICF in Brazil and South Africa –comparative data from four cross-sectional studies. Physiotherapy. 2011;97(1):17-25.
4 Van As M, Myezwa H, Stewart A, Maleka D, Musenge E. The International Classification of Function Disability and Health (ICF) in adults visiting the HIV outpatient clinic at a regional hospital in Johannesburg, South Africa. AIDS Care. 2009;21(1):50-8. PubMed PMID:19085220.