For people who can reliably access and tolerate ART, HIV is becoming a chronic and episodic condition. These cycles of wellness and illness over time are not well captured in the ICF. Therefore, the Episodic Disability Model was developed with adults in Canada to describe the unpredictable nature of living with HIV.1,2
The framework recognizes that each person living with HIV has their own disease course.
The Episodic Disability Model has 3 features:
- Dimensions of episodic disability which describe four dimensions of episodic disability and their sub-components that may be experienced by adults living with HIV (see Figure 1.4.1)
- Contextual factors of disability which describe the context in which disability is experienced. Extrinsic and intrinsic contextual factors could exacerbate or alleviate each of the four dimensions of disability for adults living with HIV (see Figure 1.4.2)
- Triggers or life events that can mark a major episode of disability (e.g., first receiving an HIV diagnosis, starting or changing medications, suffering the loss of a family member or friend) (see Figure 1.4.3)
Figure 1.4.1: Dimensions of Episodic Disability
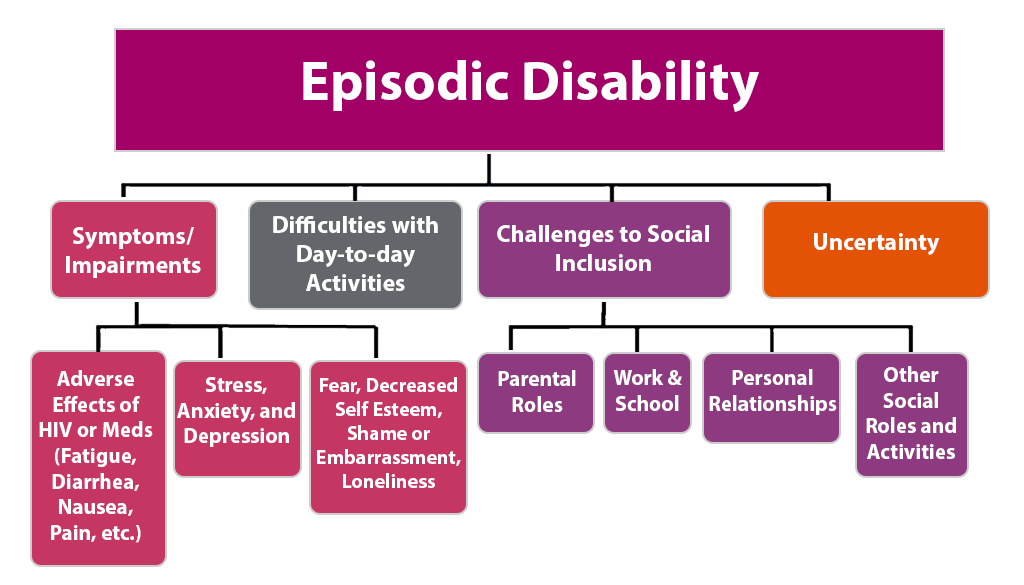
Figure 1.4.1: Dimensions of Episodic Disability – Description
This diagram shows four major dimensions of episodic disability and provides additional details for some of these categories.
The first dimension of episodic disability is symptoms and impairments. These can be caused by adverse effects of HIV or its treatment (e.g., fatigue, diarrhea, nausea, pain, etc.). They can also include stress, anxiety and depression. Symptoms and impairments can also be impacted by fear, decreased self esteem, shame or embarrassment or loneliness.
The second dimension of episodic disability is difficulties with day-to-day activities.
The third dimension of episodic disability is challenges to social inclusion. This can include challenges with parent roles, work and school, personal relationships and other social roles and activities.
The fourth dimension of episodic disability is uncertainty.
Figure 1.4.2: Contextual factors of disability
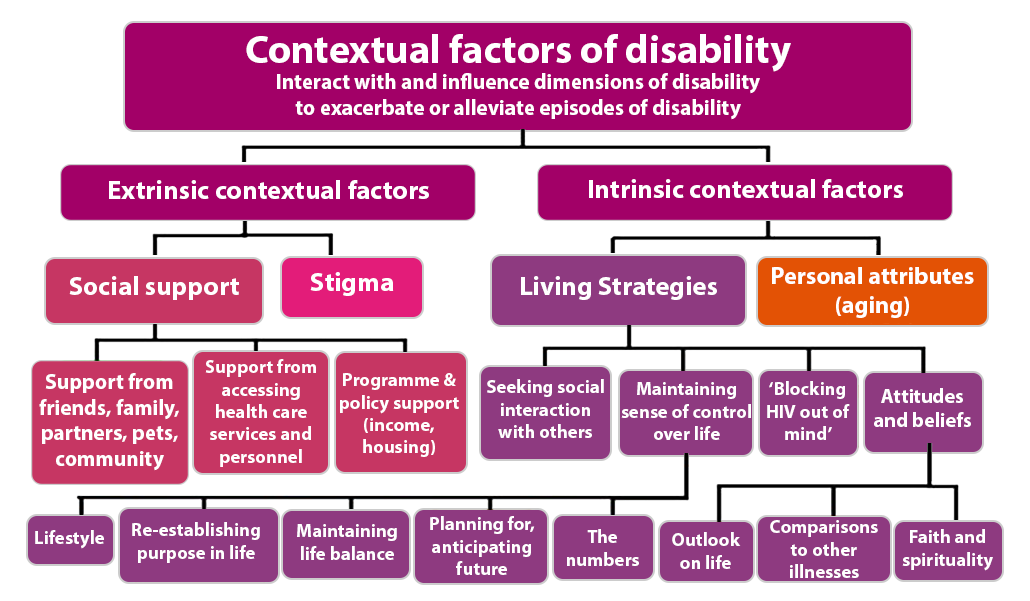
Figure 1.4.2: Contextual factors of disability – Description
This diagram shows two major contextual factors of disability. These interact with and influence dimensions of disability to exacerbate or alleviate episodes of disability.
External contextual factors include social support and stigma. Social support may come from friends, family, partners, pets or community. Support may also come from accessing health care services and personnel and program and policy supports (e.g., for income or housing).
Intrinsic contextual factors include living strategies and personal attributes (e.g., aging). Living strategies include seeking social interaction with others, blocking HIV out of the mind maintaining sense of control over life and attitudes and beliefs. Maintaining a sense of control over life may include lifestyle, re-establishing a purpose in life, maintaining life balance, planning for and anticipating the future and maintaining appropriate levels of biological markers for disease management. Attitudes and beliefs may include outlook on life, comparisons to other illnesses and faith and spirituality.
Figure 1.4.3: Triggers
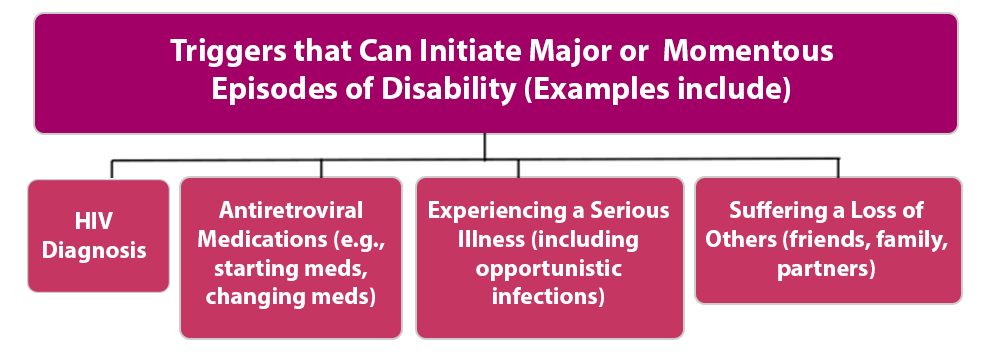
Figure 1.4.3: Triggers – Description
This diagram illustrates triggers that can initiate major or momentous episodes of disability include. These triggers may include: an HIV diagnosis, starting or changing antiretroviral medications, experiencing a serious illness (including opportunistic infections), and suffering the loss of others (e.g., family, friends, partners).
1 O’Brien KK, Bayoumi AM, Strike C, Young NL, Davis AM. Exploring disability from the perspective of adults living with HIV/AIDS: development of a conceptual framework. Health Qual Life Outcomes. 2008a Oct 4;6:76. PubMed PMID: 18834538; PubMed Central PMCID:PMC2572592.
2 O’Brien KK, Davis AM, Strike C, Young NL, Bayoumi AM. Putting episodic disability into context: a qualitative study exploring factors that influence disability experienced by adults living with HIV/AIDS. J Int AIDS Soc. 2009 Nov 9;12(1):5. PubMed PMID: 19900284.
Section 1.4.1: Why is it helpful to think about HIV as an episodic disability?
As people with access to ART live longer, the long-term impacts of HIV and its treatments (in combination with aging itself) may lead to increased prevalence of concurrent conditions, such as arthritis, fractures from osteoporosis, diabetes, some forms of cancer, and depression or other mental illnesses.1
- HIV is considered an episodic disability2,3
- The common feature of many other conditions is that they can all be episodic both in nature and impact.
- As such, people living with HIV may experience several episodic conditions concurrently, all with different fluctuations in their functioning and health.
- Thus, the need for rehabilitation is expanding to prevent or manage such disabling impacts and promote quality of life.
This approach also helps to identify policy models that promote more flexible employment or school programs that enable people with episodic illnesses to participate when their health permits without losing the opportunity when they get sick again.
1 Ernst J, Hufnagle KS, Shippy A. HIV and older adults. 2008. New York: AIDS Community Research Initiative of America.
2 O’Brien KK, Bayoumi AM, Strike C, Young NL, Davis AM. Exploring disability from the perspective of adults living with HIV/AIDS: development of a conceptual framework. Health Qual Life Outcomes. 2008a Oct 4;6:76. PubMed PMID: 18834538; PubMed Central PMCID:PMC2572592.
3 O’Brien KK, Davis AM, Strike C, Young NL, Bayoumi AM. Putting episodic disability into context: a qualitative study exploring factors that influence disability experienced by adults living with HIV/AIDS. J Int AIDS Soc. 2009 Nov 9;12(1):5. PubMed PMID: 19900284.